
How can we mitigate injuries in the growing child?
At The Youth Physiotherapy Clinic, we are seeing a growing number of children participating in both single and multiple sports, often committing a high number of training and competition hours from an early age.
“While sport plays a vital role in children’s physical, psychological, and social development, increasing participation levels and early exposure to competitive demands have also led to a rising risk of injury in youth athletes”
The term children’s sports-related injuries covers a wide range of conditions, from sudden injuries such as ligament damage and fractures to longer-term problems caused by overuse and growth-related changes. There are many factors that can increase a child’s risk of injury, including sudden or unaccustomed increases in training load, growth and maturation changes, developing movement patterns, and inadequate nutrition, to name just a few.
While injuries cannot be eliminated entirely, the key question is whether they can be reduced—and the answer is yes. This can be a complex challenge but not an insurmountable one. Below are several practical strategies that parents and coaches can implement to help minimize injury risk and give children the best possible chance of avoiding unnecessary injuries.
A. Manage training load after summer and half term breaks
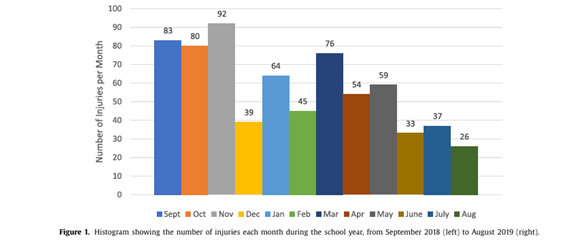
Data collected from school-aged children [Mitchell et al., 2021] highlights clear seasonal trends in injury occurrence, with distinct periods of higher and lower risk throughout the year.
“At The Youth Physiotherapy Clinic, we observe a noticeable increase in injuries between September and November, particularly following the summer break and during the return to school after half-term holidays”
During these breaks, children often significantly reduce their sporting activity; however, they then return abruptly to high training and competition loads through both school and external club sport. This sudden increase in physical demand places them at greater risk of overload-related and acute traumatic injuries.
For parents, it is worth reverse-engineering the school term and planning in advance. Planning school holidays thoughtfully can help maintain a moderate level of physical activity, which reduces the risk of a sudden spike in training volume when children return to school. In addition, communicating with schools and clubs to understand their plans for the upcoming term can help identify higher-risk areas, such as unaccustomed high-volume running, frequent fast decelerations, and a high number of impact landings.
B. Sleep
Sleep is vital for the developing child, as it is a key period for growth and tissue repair due to the high release of growth hormone. Younger children (aged 6-12) should aim for 10–12 hours of sleep per night, while older children (aged 13–18) should target 8–10 hours per night. During adolescence the bodies internal clock is delayed which can create a pinch point between the bodies biologically driven bedtime and societally imposed waketimes [school day start]. Other higher-risk situations include sports that finish late in the evening followed by early school start times.
“Relying on weekend catch-up sleep is not effective and may contribute to a chronic state of partial sleep deprivation, negatively affecting recovery and decision-making”
C. Vitamin D
Vitamin D is crucial for calcium absorption and muscle functioning. During a child’s growth they are laying down a high volume of new bone and during growth spurts the growth plates can become temporarily porous so adequate calcium absorption is key. Vitamin D also positively impacts the immune system and through this interaction can modulate injury recovery [Bouftas et al., 2024].
D. Skeletal maturation scoring
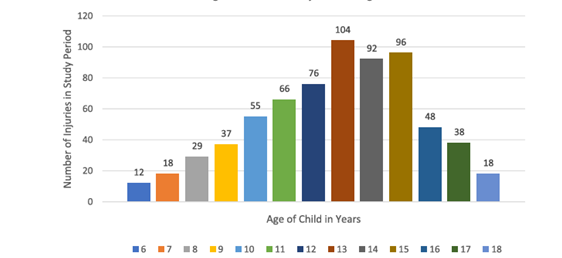
The graph above presents injury incidence by age group in school-aged children (Mitchell et al., 2021). However, such aggregated data raise more questions than they answer, including which sports are represented, whether injuries are predominantly contact-related or associated with change-of-direction demands, and whether injured athletes are specialised or multi-sport participants. A critical factor that is frequently overlooked is the distinction between skeletal age and chronological (birth) age.
Research has demonstrated that skeletal maturation may be advanced or delayed relative to chronological age, classifying children as early or late maturers (Calfee et al., 2010; Satoh & Hasegawa, 2025).
During development, children experience a period of accelerated growth known as peak height velocity (PHV), which typically occurs at approximately 90% of peak adult height. While PHV generally occurs around 12 years of age in girls and 14 years in boys, estimating maturation based on percentage of peak adult height provides a more accurate indicator than chronological age, given individual variability in skeletal maturation. The PHV phase is associated with transient disruptions in neuromuscular control, insufficient muscle capacity, and imbalances between muscle and tendon development. Evidence indicates an elevated injury risk in children who are between 88–95% of peak adult height, particularly among early maturers and those experiencing a rapid tempo of growth (Johnson et al., 2022; Monasterio et al., 2024).
Summary
Children’s sports injuries cannot be completely prevented, but they can be significantly reduced. The greatest risks occur during periods of rapid growth, sudden increases in training load (especially after school holidays), and when sleep and recovery are insufficient. By gradually managing training demands, prioritising consistent sleep, supporting bone health through adequate nutrition and Vitamin D, and considering a child’s biological maturity rather than just their age, parents and coaches can help protect growing athletes and support healthy, long-term participation in sport.
Dan is the Clinical Director of The Youth Physiotherapy Clinic in Bath
Website Youth Physio Clinic | Get Active Now — Book Today
For more information, please reach out to Dan@theyouthphysioclinic.co.uk.
References
Bouftas et al. [2024]. Vitamin D and pediatric bone health: Important information and considerations for the pediatric orthopaedic surgeon. J Paediatr Soc North Am
Calfee et al. [2010]. Skeletal and chronological ages in American adolescents: current findings in skeletal maturation. J Child Orthop, 4 (5).
Mitchell et al. [2021]. Acute musculoskeletal injuries in school age children in Britain. Injury, 52, (89).
Satoh and Hasegawa. [2025]. Factors affecting prepubertal and pubertal bone age progression. Front Endocrinol.